
In the UK, more than one in five adults over the age of 60 have peripheral arterial disease, and about 1–2% of those will develop chronic limb-threatening ischaemia (CLTI; Fu and Zhang, 2025; Houghton et al, 2024). Patients frequently present late, with tissue loss or non-healing wounds, often complicated by infection and comorbidities such as diabetes, renal disease, or heart failure (Li et al, 2022). Timely identification and referral are essential, yet service audits continue to reveal unwarranted variation in assessment, referral thresholds and patient education (Li et al, 2022).
Patient health literacy is a critical, but often neglected, component of care. Individuals with CLTI face complex treatment decisions, ranging from optimising cardiovascular risk factors and wound care to revascularisation planning and, in some cases, palliative limb management. Written information is frequently dense, technical, and poorly tailored to patient needs. Clinicians in the Society of Vascular Nurses recognised the need for concise, visual, and inclusive education resources that could be used consistently across vascular networks and broader healthcare systems.
Peripheral arterial disease
The term ‘peripheral arterial disease’ (PAD) is used to describe blockages or narrowing within the arteries caused by atherosclerotic plaque. Atherosclerosis is often generalised, and patients affected by PAD have an increased risk of fatal and non-fatal cardiovascular events (Aboyans et al, 2018). Barraclough and Bradbury (2018) describe PAD as taking a natural course from asymptomatic disease to intermittent claudication and ending for some with CLTI. There continues to be a lack of recognition at all stages of PAD, both by clinicians and patients. It is estimated that 7–15% of patients with asymptomatic disease will go on to develop intermittent claudication within 5 years (BMJ, 2025). Of patients with claudication, 25% will deteriorate further. For patients with CLTI, the prognosis is poor; 15–20% of patients will undergo a major limb amputation within 12 months, and 1-year mortality ranges from 15% to 40% (Duff et al, 2019) The estimated 5-year survival rate is 50–60% – a worse rate than most cancers (Ventoruzzo et al, 2023).
Critical limb-threatening ischaemia was defined for the first time in 1982 as rest pain and an ankle pressure of <40 mmHg, or tissue loss [Figure 1] and an ankle–brachial pressure of <60 mmHg (Jamieson, 1982). Rest pain is discomfort in the forefoot which typically occurs at night when the foot is elevated in the bed. The pain will often wake the patient from their sleep and is relieved by hanging the affected limb off the bed because gravity helps blood flow to return to the ischaemic leg. Tissue loss and necrosis occur as the blood supply to the tissues is reduced and is insufficient to maintain tissue health, resulting in cell death due to ischaemia.
In 2017, the European Society of Cardiology and the European Society of Vascular Surgery changed the term from critical to chronic , because not all CLTI patients are in a critical state requiring immediate emergency revascularisation (Aboyans et al, 2018). Sorber et al. (2023) define CLTI as the combination of ischaemic rest pain, ulceration and/or gangrene for more than 2 weeks [Figure 1]. If CLTI is not recognised or intervention is delayed, the tissue loss can significantly increase, risking limb salvage [Figure 2].
Sunset foot, or reactive hyperaemia, may be used as an assessment of arterial flow as part of the Buerger’s test. This test has two parts. Firstly, foot pallor is tested by raising both legs to an angle of 45 degrees and holding for 1 minute. Observe the colour of the feet and the angle at which they turn pale. Pallor is a sign of ischaemia and occurs when the peripheral arterial pressure is not sufficient to overcome the effects of gravity. In a limb with normal circulation, the toes and sole of the foot will remain pink, even when the limb is raised by 90°. The poorer the arterial supply, the lower the angle at which the legs have to be raised for them to become pale. A vascular angle <20° indicates severe PAD. Secondly, assess the reactive hyperaemia by asking the patient to hang their legs down over the side of the bed. Gravity will help blood flow return to the ischaemic limb. The foot will slowly turn pink and soon after red (so-called ischaemic rubor or sunset foot). This transformation occurs due to the dilatation of the arterioles in an attempt to remove the metabolic waste products that have built up in reactive hyperaemia. The foot then returns to its normal colour (Sritharan and Koufopoulos, 2023).
Risk factors for PAD include smoking, diabetes, hypertension and hypercholesterolemia (BMJ, 2023). Smoking is one of the most important preventable factors and is associated with disease progression and poor post-procedural outcomes (Behrooz et al, 2023). Liu et al. (2022) state that nearly one quarter of deaths from PAD are attributed to smoking. In addition, female sex, older age, economic status and poor access to healthcare are associated with worse outcomes in patients with PAD (Noyes et al, 2018).
The current management for PAD includes:
- Lipid management: Guidelines state all patients should be offered high-intensity statin treatment e.g. 80mg atorvastatin, if this is able to be tolerated (National Institute for Health and Care Excellence [NICE], 2020). If possible, rule out secondary causes of hyperlipidaemia prior to commencing statin treatment.
- Antiplatelet therapy: All patients with PAD should be started on clopidogrel 75mg unless intolerant or contraindicated. Aspirin can be used second line (NICE, 2020; Espinola-Klein et al, 2022;).
- Smoking cessation should be offered to reduce the risk of major cardiovascular events. This can be undertaken with behaviour support, as well as nicotine supplements if needed.
- Diabetes: A multidisciplinary approach should be taken with the diabetes team, with a target HBA1c <48mmol/mol s (Das et al, 2025).
- Exercise therapy: Patients who have limited walking distance should be offered a supervised exercise class and should be encouraged to walk to the point of maximal pain (NICE, 2020).
Best medical therapy and lifestyle changes should be managed in primary care, where clinicians can monitor adherence and offer ongoing support in a community setting where patients can access local services. All healthcare professionals in both primary and secondary care need to be aware of the symptoms of CLTI, and patients who present with leg and foot pain should have an arterial assessment performed. If CLTI is suspected, patients should be urgently referred to the local vascular units, where patients can be assessed and urgent imaging and revascularisation can be undertaken in line with the Vascular Societies’ quality improvement framework of revascularisation in 14 days (Speirs et al, 2023).
Development of the RING cards
The SVN Committee initiated the development of the RING Cards in 2023 as part of a broader programme to improve patient engagement and safety within CLTI pathways. The idea was reinforced by podiatry colleagues who requested a tool that they could give to patients with PAD to inform them about progression from chronic PAD to limb threating PAD. The aim was to produce a practical tool that could:
- Support patients and carers in recognising early warning signs of deterioration.
- Reinforce key messages shared during vascular consultations.
- Standardise the information provided across services.
- Promote shared decision-making and self-care confidence.
- Empower prompt access to vascular services.
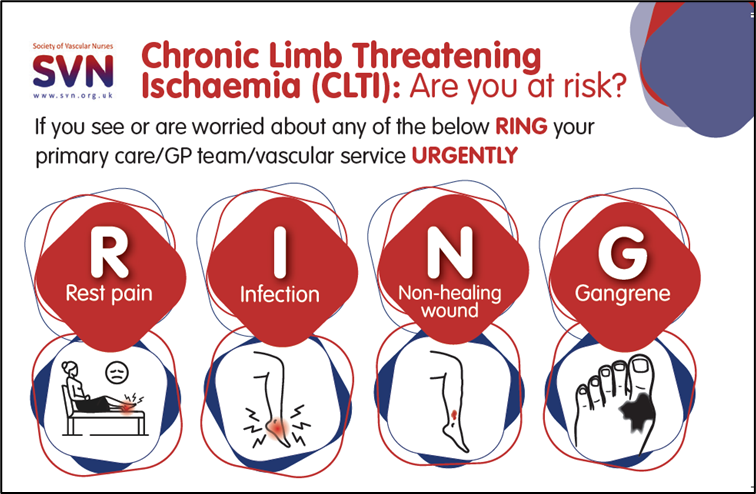
The acronym RING was selected to reflect the core message of the signs of CLTI while reinforcing urgency and patient activation:
- Rest pain.
- Infection.
- Non-healing wound.
- Gangrene.
The development followed a structured process:
Evidence review to examine international guidance on patient information for PAD and CLTI. The Circulation Foundation provides a range of patient information leaflets on PAD, but the emphasis is on diagnosis, long-term management and improving outcomes through risk factor reduction and lifestyle modification. There was a gap in patient information around the progression of stable PAD to CLTI. Yet the evidence suggests that accessing time-critical vascular assessment and intervention will improve patient outcomes, including reduced amputation rates in patients with CLTI (Boyle et al, 2022).
Stakeholder engagement: input from vascular nurses, podiatrists, surgeons, and patient-experience representatives was sought. There was consensus among the stakeholder group that the CLTI tool would be beneficial. The initial design collated the information each group felt was important and reiterated the message of time-critical assessment and intervention.
Content drafting: The creation of short, plain-language statements supported by icons and colour coding was developed using a Delphi technique until consensus was reached.
Design and testing: The pilot review took place in several vascular clinics across the UK to ensure clarity, cultural sensitivity and readability.
National launch: Hard copies were sent to all SVN members and to other clinicians who expressed an interest. The resource was hosted on the SVN website as a free download for print or digital use [Figures 3 and 4].
Implementation and use in practice
Dissemination of the cards initially began within vascular nurse specialist clinics and vascular surgeon clinics, later extending to wound care and podiatry services. This approach ensured consistent messaging across multiple disciplines and care settings, reinforcing patient understanding of the time-critical nature of early recognition and detection of complications associated with PAD. Integrating card distribution into established clinic pathways allowed seamless alignment with existing patient education pathways. More importantly, it created opportunities for shared decision-making conversations between clinicians, patients and carers, supporting informed choices and proactive management in the event of progression of limb ischaemia.
Potential impact on patient outcomes and service quality
A simple patient-held ring card that shows early indications of PAD can improve self-management and reduce time delays in detecting ischaemia. Early symptom assessment and prompt referral are critical to reducing ulceration, infection, and limb loss, with late presentation still a key driver of major amputation in the UK (Conte et al, 2019; National Wound Care Strategy Programme, 2024). The card directly addresses acknowledged deficiencies in patient understanding, which are widespread in PAD due to low health literacy and the significant burden of multimorbidity (NICE, 2020).
The ring-card format provides an easily available visual resource aimed at enhancing the reading age and improving independence, language hurdles, and socioeconomic variation, factors that have frequently been found to contributing to disparities in vascular outcomes (Public Health England, 2019). Standardised education tools like these directly assist national aims, since the NHS Long Term Plan promotes tailored treatment, supported self-management, and the avoidance of unnecessary disparities (NHS England, 2019).
Preliminary feedback from patients reveals a better understanding of worrying symptoms and more alertness when monitoring limb changes. Community nurses report more timely re-referrals to vascular services, indicating quicker escalation and less deterioration before review.
The card has also made communication better by giving patients, families, and doctors a common point of reference. It has also helped reduce anxiety after discharge by giving clear instructions on when to ask for help.
The tool will help improve independence in early recognition of PAD symptoms by standardising teaching messages across multidisciplinary teams. These benefits may have an impact on limb salvage rates, wound healing times, and unplanned readmissions, which is consistent with evidence that structured patient education improves vascular outcomes when integrated into pathway-wide service design (Bridgwood et al, 2020).
Although no formal evaluation has yet been undertaken, early qualitative feedback suggests several benefits:
- Improved understanding and vigilance: Patients more readily identify the symptoms of deterioration, such as increasing pain or colour change.Timelier escalation: Community nurses report reduced delays in re-referral to vascular teams.
- Enhanced communication: The cards provide a common language between patients, carers, and professionals.
- Reduced anxiety: Clear instructions reduce uncertainty following discharge.
- Standardisation of education: Aligns messages across multidisciplinary teams and reduces regional variation.
Collectively, these improvements have the potential to influence clinical outcomes, including limb-salvage rates, wound-healing times, and unplanned readmissions.
Conclusion
CLTI remains a time-critical, high-mortality condition in which delays in recognition and referral can result in avoidable limb loss and death. Despite clear clinical pathways, many patients continue to present late, highlighting a persistent gap in patient understanding of disease progression and warning symptoms. The development and early implementation of the Society of Vascular Nurses RING Cards was a simple, pragmatic response to this challenge.
By translating complex clinical information into clear, visual, patient-centred messaging, the RING Cards support health literacy, reinforce consultation discussions, and promote timely patient activation when symptoms deteriorate. Early feedback suggests the cards enhance confidence, reduce uncertainty and facilitate faster escalation back into vascular services, supporting more equitable and standardised education across care settings.
While formal outcome evaluation is ongoing, the RING Cards represent an important step towards embedding patient empowerment within CLTI pathways. As healthcare systems continue to address unwarranted variation and late presentation, scalable educational tools such as these have the potential to contribute meaningfully to improved limb salvage, patient experience, and service quality. Empowering patients to recognise risk and act promptly should be considered a core component of contemporary vascular care, rather than an adjunct to it.



