Malignant wounds are defined as those that occur as a result of cancer, either caused by the disease itself or as a complication of cancer treatment (e.g. radiotherapy). Malignant wounds may also be fungating, which occurs when cancers grow and break through the surface of the skin, creating a wound (Ousey et al, 2024). While malignant wounds may be present for long periods of time, they often develop during the last months of life and can be an indicator of the impending end of life (Alexander, 2010). Therefore, palliative care, with a focus on preserving comfort, dignity and quality of life (QoL) as much as possible, is generally the appropriate course of action for these wounds (Starace et al, 2022).
Malignant wounds can be devastating for patients and their families, and can be difficult and distressing for the HCPs managing them. In end-of-life patients, it can be psychologically difficult for HCPs to adjust to the concept that healing may not be the aim, or may not be possible. The distress that individuals and their families, friends and carers may be experiencing may also be distressing or upsetting for the HCP (Ousey et al, 2024).
The European Wound Management Association document ‘Palliative wound care: Recommendations for the management of wound-related symptoms’ (2025) highlights that, despite advancements in wound care, there remains a lack of ideal dressing options for palliative wounds and many advanced wound dressings are not available in sizes or configurations suitable for these wounds. Many advanced wound dressing designs are based on the concept of moist wound healing (Liang et al, 2023), which was primarily developed for acute wound management, and may not translate effectively to palliative wounds.
Background
This case study is presented from the viewpoint of the nurses working in a hospice setting, providing care and support for a patient in their last months of life. The patient’s thoughts and words have been captured with consent to share with a wider audience, supporting education around palliative wound care (PWC). PWC is a comprehensive approach to managing symptoms for vulnerable patients with a low QoL and focuses on delivering person- and family-centred interdisciplinary care (Lee et al, 2022). The ‘palliation of wounds’ is a recent approach that requires a different mindset than conventional wound care (Alvarez et al, 2016).
This case study also highlights the use of HidraWear (a dressing retention system), when standardised care could not provide effective symptom control for this patient.
Judy’s story*
(*Name changed for confidentiality)
Judy was diagnosed with colorectal cancer at the age of 42. She underwent a surgical bowel resection in 2018 and, due to obstructive uropathy, JJ ureteral stenting. In 2020, the cancer had returned, with metastases to the liver, and a liver resection was successfully performed. In 2022, further metastatic cancer was identified in the lung, and a right lobectomy was performed. A new pelvic tumour within the bowel presented 12 months later and Judy received multiple cycles of chemotherapy and radiotherapy.
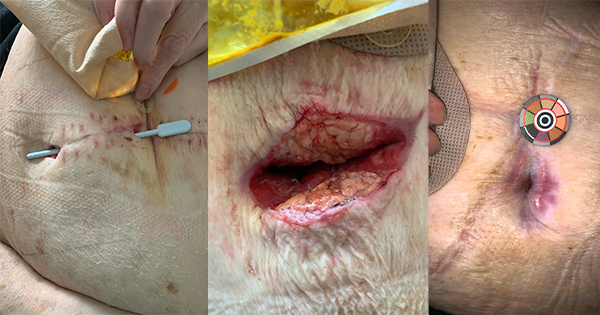
At this point, a wound to the lower back was identified. This initially presented as necrotic tissue, alongside symptoms of lower back pain and sensation changes in the lower legs. Magnetic resonance imaging (MRI) showed spinal cord compression due to a tumour, presenting as an MFW. The most common cause of MFW is advanced cancer infiltrating the skin and blood vessels (Grocott et al, 2013), which requires a PWC approach (Sezgin et al, 2023).
The wound to the lower spine increased in size. The full extent of the depth was not established; however, it involved fistulae into the bowel and was suspected to extend into the vaginal region. A fistula refers to a tubular linkage between two hollow organs or between a bodily cavity and the external surface (Bryant and Nix, 2016), which can be caused by the presence of a rapidly proliferating tumour.
The cancer with metastases was incurable, therefore palliative care planning commenced with Judy and her family. Palliative care refers to a team-based approach focused on preventing and relieving patient suffering and improving the patient’s QoL by managing physical, psychosocial and spiritual concerns (Meier et al, 2017).
Hospice palliative care provision
Judy was admitted from secondary hospital care to a hospice ward for palliative symptom management, which included PWC. She remained in hospice care for the last months of her life.
People with MFW can experience distressing symptoms (such as pain, odour, exudate, bleeding, infection and pruritus), which can have detrimental effects on their physical, psychological and functional health during their last days of life (Grocott, 2000).
The nursing staff at the hospice built a strong nurse-patient relationship with Judy and were committed to providing person- and family-centred care. They described Judy as a vibrant 49-year-old wife and mother, who had a great presence and loved nothing better than browsing online fashion clothing sites, ordering colourful shoes and applying red lipstick every day, despite her prognosis and the effects of chemotherapy and radiotherapy treatment on her wellbeing. For every patient with a terminal diagnosis, an individualised approach is key to ensuring high-quality, safe and person-centred care (Russell et al, 2024).
During this period, Judy’s predominant symptoms were directly related to the MFW on her lower spine, which was leaking large amounts of wound exudate. Additionally, due to the tracking fistula into the bowel, the wound exudate was mixed with faeces, causing moisture-associated skin damage (MASD). The JJ urostomy stent also became blocked, causing urine to leak onto the skin, exacerbating the MASD and increasing pain to the site during cleansing and wound management.
MASD causes overhydration of the skin from urine, faeces, sweat, or saliva and disrupts the barrier properties of the stratum corneum, allowing irritants to penetrate the epidermis, and making the skin more prone to physical damage, including friction and shear (Beeckman et al, 2015).
Exudate management is a critical aspect of wound care, particularly in palliative settings where heavy leakage is common in cases of MFWs, especially if necrotic tumour outgrowths or fistulas are present. These factors can complicate wound management and increase patient distress (Chrisman, 2010). Fluid drainage from fistulas also presents unique challenges, requiring strategies to minimise odour associated with fistula discharge.
Impact of palliative wound care management
Interventions for removing dressings, cleansing the skin and reapplying absorbent dressings were extremely traumatic for the patient, her family and the HCPs involved. Dressing removal could take up to 3 hours, as the pain was so severe. Staff were often allocated to provide PWC only for this patient during their shift, to provide continuity and maintain the trusted relationships established with Judy and her family.
A lack of continuity in symptom management frequently leaves patients feeling confused and lost (Basile et al, 2024) and also impacts on HCPs, leading to support being necessary. Wilkes et al (2003) conducted semi-structured interviews with nurses caring for people with wounds of this kind, and highlighted difficulties for nurses in the following:
- Applying dressings
- Coping with odour
- Managing emotional strain.
When HCPs entered her room, Judy would instruct them: ‘please don’t talk about the wound, just get on with it [the dressing management process]’. She often cried, not only from pain (despite pre-procedure analgesia), but due to the odour and super-absorbent pads applied to the area, which she likened to wearing a bulky continence pad. It should be noted that Judy felt her wound was the worst element of her cancer journey. In particular, she experienced fear and embarrassment due to exudate leaking through dressings onto her clothes and bedding. In palliative care, it is particularly important for patients to feel understood, heard and treated as capable individuals (Klarare et al, 2013), focusing on the elements of care that are most important to them.
The odour from the wound was very strong and could be smelled outside the room, reaching into the corridor. Visitors often commented as they came onto the ward, which Judy sometimes overheard; this caused her to want to be isolated. Wound odour is cited by both patients and HCPs as one of the most challenging and distressing symptoms associated with malignant wounds (Woo et al, 2015). This can cause isolation, depression and reduced QoL (Gethin et al, 2023). In malignant wounds, malodour may be caused by bacteria, high levels of exudate or poorly vascularised tissue, which allows aerobic and anaerobic bacteria to rapidly proliferate and decompose serum proteins present in the wound fluid (Niculescu et al, 2024). Various approaches, such as cat litter trays, odour-absorbing dressings and scented candles were tried, but proved ineffective.
For Judy and her family, movie nights were a big treat. The one thing she wanted was to go out to the cinema wearing her skinny jeans. However, the wound dressings were too bulky and uncomfortable, and Judy described herself as feeling ‘ugly and disgusting’. As the dressings had such an impact on Judy, the nurses planned her dressing change routines to be as non-invasive as possible, timing them around her children’s visits after school. However, the wound dressings used led to further complications. Adverse reactions to adhesives and silicone-bordered foam dressings caused skin excoriation and medical adhesive-related skin injury (MARSI). Koumaki et al (2023) emphasised the lack of clinical evidence to guide dressing choices, leading to guidelines based on majority opinion and case studies.
The turning point: HidraWear
One of the hospice nurses attended a wound care event and witnessed a presentation on a dressing retention system, HidraWear, which was originally designed for exuding wounds caused by the condition hidradenitis suppurativa (HS). HS is a chronic inflammatory skin disease of the hair follicle, which can lead to abscesses and tunnelling lesions with high exudate volumes on areas such as axillae, groin, abdominal folds, buttocks and under the breasts (Schofield, 2024).
By being simple and easy to use, HidraWear aims to achieve a balance between HCP and self-care provision. An absorbent non-adhesive dressing manages exudate, and is kept in place by soft dressing retention baselayer that look like regular clothing. The absorbent non-adhesive dressing is placed inside the dressing retention baselayer under specially designed perforations and retained by a SecureLock™ Technology Fixation Tab.
A study evaluating ease of use and impact on QoL concluded that HidraWear had a significant positive impact on QoL, particularly regarding some of the most distressing and challenging factors associated with HS: pain, discharge, comfort and time constraints (Moloney et al, 2022).
The hospice team discussed the potential benefits of HidraWear for Judy and agreed to incorporate it into her PWC. HidraWear was sourced and care planning adjusted accordingly. The immediate impact, according to the nurses, was ‘life-changing’. They described it as ‘unbelievable’, ‘the best thing [they] had experienced in 30 years of nursing’, and stated that ‘it changed everything’, with Judy’s QoL improving instantly.
The pain levels associated with her wound reduced, as no adhesives were used to retain the dressing; pre-dressing analgesia was eventually stopped. Within 1 week, the surrounding skin, previously damaged by MASD and MARSI, had healed. The number of daily dressing changes was reduced to two, with ease of removal and application with the Velcro fastening.
Judy’s wish to go to the cinema with her family became a reality in the last two months of her life. Using HidraWear, she was able to wear her beloved skinny jeans without feeling bulky and uncomfortable; she described it as feeling ‘like wearing support underwear, safe and secure’.
Nurses’ reflection
The mission of palliative care nursing is to reduce pain and give the patient the best death possible. At the start of Judy’s treatment, we were not achieving this, as she was in significant pain, and we went home at night feeling that we were not doing enough. All staff dreaded the time for dressing changes as, whatever we tried, nothing succeed in either speeding up the process or minimising her pain. This was draining and disheartening for staff.
In the study by Wilkes et al (2003), nurses described malignant wounds as being difficult to manage, frequently personally distressing and often leading to feelings of guilt or inadequacy if they had not been able to manage the wound in a manner they considered acceptable. They were particularly affected when caring for somebody of their own, or their parents’, age or when young children were involved.
The experience for student and junior nurses can be particularly difficult. We don’t often see cancer growing or spreading, as this typically happens inside the body, but in malignant wounds, the disease process is visible and this can be quite shocking to witness. As a team, we reflected that the wound is often viewed as additional in palliative symptom management. We noticed comments from the medical team when viewing the wound, such as ‘it’s increased in size’ or ‘it has deteriorated’ – language that had a negative impact on the patient. Words used to describe the wound should be chosen carefully, remaining factual and avoiding terms that might be upsetting for the patient (Ousey et al, 2024).
Although Judy understood her prognosis, emotionally the wound became her primary concern. Integrating wound management into end-of-life care planning ensures that wound care aligns with the broader goals of palliative care. Discussions about wound care should include input from patients, families and interdisciplinary teams, ensuring that interventions prioritise comfort and dignity while addressing both the physical and emotional dimensions of care (Sezgin et al, 2023; Schubert et al, 2022).
Guidance for practice
Malignant wounds can be extremely challenging for HCPs. There is a need for increased awareness and education surrounding this wound type, to support both HCPs and patients.
The consensus document ‘Malignant wounds: Management in practice’ (Ousey et al, 2024) provides practical guidance and tips for managing malignant and fungating wounds, including effective communication with patients and their families. The document includes the POSIES clinical support pathway, which provides specific guidance for practice [Figure 1].
Conclusion
With the predicted increase in cancer incidence (Vardhan et al, 2019), the prevalence of MFWs is likely to increase, consequently escalating healthcare demands (Kaasalainen et al, 2020). Nurses need education, knowledge, adequate resources, time, and emotional support to effectively manage these challenging wounds. This support should include a safe environment where nurses can express their emotions, aiding in the prevention of feelings of hopelessness, failure and fear in managing MFWs (Russell et al, 2024).
A patient’s wound care plan must involve collaboration with clinical specialists, including tissue viability nurses and pain management experts, to alleviate the severe symptoms associated with MFWs (Qiu and Good, 2021). It is imperative that HCPs address all aspects of physical, social, psychological and economic care to enhance the QoL of patients receiving PWC, reaffirming that the patient’s needs are paramount (Gethin et al, 2020).
Judy’s case highlights the importance of individualised care that prioritises what matters most to the patient. The introduction of HidraWear to her care plan significantly improved her QoL, allowing her to enjoy meaningful experiences at the end of her life, experiences that fulfilled her wishes and created lasting memories for her family.