Cavity wounds are characterised by a loss of tissue that extends beneath the surface of the skin, resulting in a hollow pocket or cavity within the wound bed (Tickle, 2025). Cavities can form within a range of wound types, often arising after significant tissue trauma (for example from surgical wounds, pressure wounds or other injuries), chronic diseases (such as diabetes and vascular conditions) or infection that leads to deep tissue destruction. Other contributing factors such as malnutrition, dehydration and immunosuppression from underlying disease or medication can further impair wound healing (Powers et al, 2016; World Union of Wound Healing Societies [WUWHS], 2019; Tickle, 2025).
Importantly, suboptimal management of complex wounds can also increase the likelihood of cavity formation and static wound healing, leaving the patient vulnerable to further damage of deep tissues and internal structures, at risk of infection and with a compromised quality of life (Tickle, 2025). Clinicians must therefore be equipped to identify, assess and accurately document cavity wounds during clinical evaluation, as well as understand the range of advanced dressing technologies available to support the unique needs of each presentation (Smith et al, 2015).
Complex cavity wounds
Cavity wounds are inherently complex and according should always be treated as such. Those involving or exposing underlying structures such as bone, muscle or even organs typically require specialist referral. The hollow cavity, often termed “dead space” in the wound bed, can trap exudate and support microbial growth, increasing the risk of deep tissue infection and biofilm formation during exudate pooling. Exudate pooling can also contribute to maceration of surrounding tissue (Timmons and Johnstone, 2022; Wounds UK, 2025).
Cavity wounds often possess hidden architectures formed by tissue erosion such as tunnelling, undermining or sinus tracts which, left unmanaged, can contribute to further tissue destruction and higher risk of infection. To identify such architectures and assess the true extent and depth of the wound, advanced imaging techniques or ultrasound may be required (Wounds UK, 2025).
Management of cavity wounds
The management of cavity wounds in the UK follows a structured clinical pathway, typically led by community nursing teams in collaboration with tissue viability nurses (TVNs) (Wounds UK, 2025). Treatment decisions are informed by national guidance, including NICE recommendations, local NHS formulary protocols and best practice statements from Wounds UK (Gloucestershire Wound Care Dressing Guidance, 2024; NICE, 2019; Wounds UK, 2025).
Initial wound assessment is essential to guide dressing selection and the overall treatment strategy. This includes evaluation of wound depth, shape, undermining, tunnelling, exudate volume, the condition of the surrounding skin and any signs of local or systemic infection such as malodour, bleeding, warmth, swelling, discharge or new pain (Brown, 2022). To support consistent and comprehensive clinical assessments, frameworks such as TIME (Tissue, Inflammation/Infection, Moisture, Edge) and the Applied Wound Management assessment scale are widely used (Smith et al, 2015). These tools help clinicians accurately document tissue types (necrotic, sloughy, granulating, epithelialising) and guide appropriate intervention.
Wound cleansing is typically undertaken with sterile saline or a wound irrigation solution, followed by debridement – the removal of devitalised or infected tissue to promote healing. Several methods are used depending on clinical judgement, including surgical debridement (rapid but non-selective), high-pressure irrigation and autolytic debridement, supported by dressings such as hydrogels, hydrocolloids or alginate-based products (Smith et al, 2015; Wounds UK, 2022). Autolytic methods maintain a moist wound environment that encourages the body’s own enzymatic processes to soften and remove slough.
Dressing selection should be based on the characteristics and needs of the wound as well as patient comfort and tolerability. For example, calcium alginates are useful in bleeding and exuding wounds due to their absorptive capacity and ability to conform to deep cavities (Smith et al, 2015). Conversely, absorptive fiber-based dressings are not recommended for use on dry or necrotic wounds (Gloucestershire Wound Care Dressing Guidance, 2024).
Recent best practice guidance cautions against the overpacking of cavity wounds, a risk associated with the traditional practice of “packing”. Overpacking may result in pressure injury, maceration, pain or stagnation of healing (Timmons and Johnstone, 2022; Gloucestershire Wound Care Dressing Guidance, 2024). Instead, the term “filling” is preferred, as it emphasises the gentle placement of conformable, pressure-free materials that fill the dead space without exerting force on the wound bed or surrounding tissue. This approach supports healing from the base of the wound upwards and reduces the risk of complications associated with overpacking (Wounds UK, 2025).
When infection or bioburden is suspected, antimicrobial dressings may be used, including silver, iodine, medical-grade honey or enzyme-based products. For deep wounds, systemic treatment is also required (Powers et al, 2016). For wounds that remain static or produce high levels of exudate, negative pressure wound therapy (NPWT) is often introduced. NPWT is widely used across NHS services to accelerate granulation, manage moisture and reduce microbial load (Smith et al, 2015). It is often used in conjunction with cavity-appropriate topical agents such as Flaminal® (Flen Health®), which can be applied directly into the wound bed to provide antimicrobial protection, manage exudate and support autolytic debridement (Flaminal® Instructions for Use, 2021).
Flaminal® is a primary dressing categorised as an enzyme alginogel used to support the management of cavity wounds, among other exuding wound types. Its multimodal action combines exudate management, autolytic debridement and antimicrobial protection via a patented enzyme system (glucose oxidase and lactoperoxidase) that provides antimicrobial protection to a broad spectrum of microbes (Beele et al, 2012; Yousefi et al, 2022; Costella and Pranjic, 2023).
The alginogel base absorbs exudate, and facilitates autolytic debridement, supporting the removal of slough and necrotic tissue, which, if left unmanaged, can increase the risk of infection.
Flaminal® is able to conform to irregular wound architecture, filling the dead space in the wound cavity and tunnels. This is an important factor in preventing exudate accumulation, minimising infection risk and promoting effective tissue regeneration (EWMA, 2007; Beele et al, 2012; WUWHS, 2019).
Two formulations are available: Flaminal® Hydro, for slight to moderately exuding wounds, and Flaminal® Forte, for wounds with moderate to high levels of exudate. Flaminal® is particularly well suited to cavity wounds due to its gel consistency, which allows for direct application without the need for traditional ribbon packing, improving patient comfort and simplifying dressing changes. Both formulations of Flaminal® provide antimicrobial protection, protect the surrounding skin and promote progressive granulation within the cavity (Costella and Pranjic, 2023).
Case 1 – Embracing change
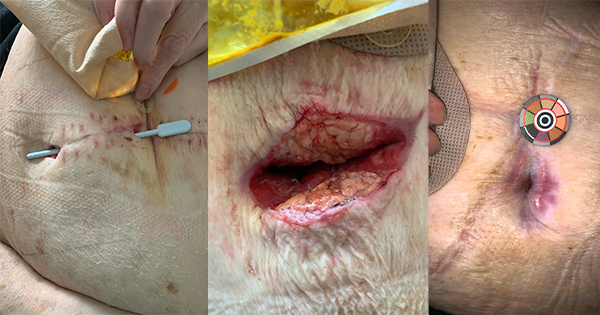
A 75-year-old woman with a history of hypertension developed partial wound dehiscence at two points along her abdominal surgical scar following emergency laparotomy and ileostomy for large bowel obstruction.
At week 1, she was initially managed with daily packing using a fiber-based ribbon, but there was minimal healing progress. Over the following two weeks, the wound sites deteriorated, with increasing slough, odour and the development of a sinus tract measuring 8cm in depth. Tunnelling formed between the two sites and local infection was suspected. By week 4, the surgical team performed a small incision to connect both wounds into a single cavity. On the final visit from the Acute Community team, it was documented that the alginate rope dressing had “become gel-like and stuck to the base of the wound”. This made removal difficult and highlighted the limitations of fibre dressings in managing exudate, as well as the potential infection risk and need for possible surgical intervention to remove retained dressing material.
The patient was then referred to the district nursing and tissue viability teams, and the dressing regimen was changed to Flaminal® Forte in combination with NPWT. At week 5, one week after starting this new regimen, the wound circumference had reduced by 22%, and depth had decreased by 1cm. Granulation tissue was visible and dressing frequency was reduced. A short reintroduction of ribbon to deliver topical steroid was associated with increased wound depth, which resolved after returning to Flaminal® Forte and NPWT. By week 14, the wound had reduced to 0.3cm² with a depth of 2.5cm, and complete healing was achieved by week 17. Flaminal® Forte supported wound bed debridement and exudate management, was well tolerated and allowed for extended wear time. Compared to prolonged use of a fiber-based ribbon dressing in the first three weeks, this combined approach was associated with improved healing outcomes and greater cost-effectiveness.
Case 2 – Reducing sandwich dressings
A 71-year-old woman with a history of hypertension was referred to community nursing services following emergency abdominal surgery and formation of an end ileostomy. Although the hospital discharge summary mentioned a sacral pressure ulcer and thromboprophylaxis, it omitted reference to two open cavity wounds on the abdomen, which were discovered by the community nurse at the initial visit (week 1). These wounds were presumed to be the result of surgical dehiscence.
Initial documentation was limited, and the wound beds were not assessed for depth due to lack of probing equipment. Early reviews recorded undermining at both sites (3cm at the lower wound and 2cm at the upper wound), but the wound base remained obscured and visibility poor. The first weeks of management involved daily application of fibre-based rope dressings, with minimal changes to technique and limited signs of healing.
By the second week, undermining remained unchanged, with persistent maceration and poor periwound skin condition. At this stage, Flaminal® Forte was introduced in combination with the existing dressing to reduce slough and support wound bed preparation. This was followed by visible periwound contraction and a reduction in wound circumference. However, by the end of the week, wound deterioration was documented, including tracking to 4cm in the lower wound and extensive undermining at 12 o’clock in the upper wound, now measuring 15cm. Ongoing use of fibre-based dressings was linked to wound tension and maceration.
In week 3, Flaminal® Forte monotherapy was trialled as a new approach, applied directly into the cavity without internal packing. This coincided with measurable improvement.
By week 4, the upper wound had reduced to 0.9cm² in area with 1cm depth and the lower wound was recorded at 0.7cm² with minimal depth and persistent undermining. The upper wound was deemed healed and undermining in the lower wound had resolved by week 6. A temporary reintroduction of rope dressing coincided with wound stagnation and increased depth. Once Flaminal® Forte monotherapy was reinstated, healing resumed rapidly: undermining reduced to 1cm, then resolved fully, with external circumference reducing to 0.29cm². By week 7, both sites were fully healed.
Flaminal® Forte was well tolerated by the patient and supported exudate management and autolytic debridement, providing a clean wound bed for granulation within the cavity.
When used alone, it was associated with improved wound visibility, reduced undermining and rapid contraction. In contrast, extended use of fibre dressings appeared to contribute to delayed healing, internal tissue pressure and dressing-related discomfort. This case illustrates that in select patients without systemic complications, Flaminal® Forte alone may be sufficient to support cavity wound healing without requiring negative pressure therapy.
Case 3 – Reducing the bulk
A 72-year-old woman with a background of hypertension and hypercholesterolaemia was referred to community nursing services following an elective ileostomy reversal. Although the hospital discharge summary stated that there were no complications and included instructions for daily wound care, the patient presented with a cavity wound measuring 3cm in depth and 4cm of undermining. The wound had been packed with ribbon dressing on discharge and was initially re-dressed in the community using the same approach, secured with an adhesive secondary dressing.
In the first week post-discharge, the dressing regimen involved twice the volume of ribbon packing compared to the initial hospital application, although the rationale for this escalation was not recorded. By day 6, the wound remained 3cm deep with unchanged undermining. A swab result subsequently revealed a heavy growth of Escherichia coli and oral antibiotics were prescribed. Despite this, wound width increased to 2.5cm and surrounding tenderness escalated, prompting concerns about dressing-related tension. Minor periwound trauma was noted and several potential suture remnants were observed at the wound edge.
After over a week of static healing and increased discomfort, a thinner ribbon dressing was trialled alongside a switch to negative pressure therapy. Within two days, the wound area reduced from 2.8cm² to 2.5cm² and undermining decreased to 3cm. The wound continued to progress rapidly over the next two weeks, with depth reducing to 2cm, undermining resolving and external measurements dropping to 1.1cm². At this point, the dressing regimen involved negative pressure therapy without internal packing.
Although brief reintroduction of internal filler led to a minor increase in undermining, once the wound was again managed without internal dressings, healing resumed. The site eventually healed fully by week 7 and the patient was discharged from care. This case highlights how reducing internal dressing bulk in cavity wounds, particularly where infection or tension is present, can relieve pressure, enhance patient comfort and accelerate healing.
Case summary
Cavity wounds in community and post-surgical care settings are becoming increasingly complex, with greater variability in wound depth, undermining and patient comorbidities. These three cases highlight the importance of early and appropriate dressing selection in driving healing outcomes and optimising resource use.
In each case, fiber-based rope or “sandwich” dressings were initially used to manage wound cavities. However, the use of combined or layered dressings was associated with delayed healing, increased tissue tension and greater patient discomfort. When Flaminal® Forte was used alone, without additional internal packing or sandwich dressings, patients experienced more rapid wound contraction, improved comfort and fewer dressing changes. This approach also reduced the risk of overpacking and product retention and was linked to faster resolution of undermining and dead space. The cases suggest that, in appropriate patients, Flaminal® Forte monotherapy may be preferable to combined dressing techniques, offering both clinical and cost benefits by streamlining care and reducing the need for multiple products.
In Case 1, the extended use of ribbon contributed to wound deterioration and delayed the initiation of NPWT. It was documented that the alginate rope dressing had become gel-like and stuck to the base of the wound, making removal difficult and underscoring a key limitation of traditional ribbon dressings in managing highly exudating wounds.
Patients also reported discomfort during dressing changes, and the overall impact on wound progression, patient experience and costs was notable. Flaminal® Forte, selected for its suitability in managing moderate to highly exuding cavity wounds, was introduced either alone or in combination with NPWT. Its absorbent gel matrix and enzymatic antimicrobial system supported wound bed debridement, antimicrobial protection and moisture balance. All cases showed visible clinical improvement within the first two weeks, with reduced undermining, fewer dressing changes and eventual complete healing. Overall, these cases underline the need for clinicians to critically assess default practices and tailor dressing selection to the specific needs of complex wound presentations.
Insights from TVNs and Community Nurses
Recent interviews with TVNs and senior community nursing staff from Essex University Partnership Trust highlight the increasing complexity of cavity wound care in community settings. Referrals for such wounds are now received every 1–4 days, underscoring the routine burden these presentations place on district nursing services.
While there was broad agreement that wound complexity has increased (100% of respondents), there was a divide over whether staff feel adequately trained and supported in managing these wounds (50% agree, 50% disagree). Inconsistent education and variable practice remain ongoing challenges, with a recognised need for clearer guidance and skill development.
Fiber-based ribbon dressings remain the most commonly used product for cavity wounds (100% of respondents), particularly those deemed “simple” (≤4cm deep, no infection or tunnelling). However, some TVNs expressed concern that this default approach may not always align with clinical need. Enzyme-based alginogels were cited by several clinicians as more practical, better tolerated by patients and easier to apply.
Patient experience also emerged as a key theme. Up to 85% of nurses reported that patients “sometimes” or “often” experience discomfort during cavity dressing changes. Contributors to pain included overpacking, lack of analgesia planning and repeated use of traditional dressings not tailored to wound depth or exudate. This discomfort can impact dignity and contribute to patient reluctance during treatment.
Expectations for healing were generally consistent, with most staff anticipating resolution of uncomplicated cavity wounds within 4–8 weeks, with the exception of 17.2% of respondents who estimated longer than 8 weeks. Some respondents cautioned that inappropriate product selection and delays in escalation can unnecessarily prolong healing.
Systemic barriers to optimal care were also noted, including caseload pressures, limited product awareness and fragmented implementation of newer technologies. Respondents agreed that delays in healing are more often the result of service limitations than patient behaviour.