
Wound debridement is a fundamental, evidence-based process in wound management. It is well known as the removal of all non-viable tissue as part of wound bed preparation to promote wound healing (Gray et al, 2011; Vowden et al, 2011).
Mayor et al (2024) have proposed an updated, more concise description of debridement as ‘the removal of viable (living) and non-viable wound components, including necrotic tissue, slough, microorganisms, biofilm, extracellular polymeric substance (EPS) and foreign materials.’
Wound hygiene measures including debridement, exudate management, the use of non-antimicrobial agents and early intervention, are essential for reducing bioburden and preventing infection. Collectively, these approaches can help reduce reliance on systemic antimicrobial medications (Blackburn et al, 2025).
Why is debridement important?
Debridement stimulates healing by promoting an optimal wound environment, reducing the risk of infection and draining areas of pus or collections. It also allows inspection of deeper structures to tailor care plans and facilitate the taking of deeper samples for culture. Furthermore, debridement can encourage pinpoint bleeding, which stimulates granulation tissue formation. Debridement of the wound periphery removes callus, reduces pressure, and enables cell migration. In addition, it optimises the action of topical dressing regimens, improves patient quality of life and reduces wound management costs for the NHS (Gray et al, 2011; Vowden et al, 2011; Chadwick et al, 2014; Murphy et al, 2020; Mayor et al, 2024).
Clinical decision-making and competency
There are many forms of debridement available, and a full holistic patient assessment must be performed prior to selecting any method of debridement to reduce the risk of complications. The chosen approach depends on the knowledge, skills and competency of the treating healthcare professional, which vary according to training and experience. All healthcare professionals should keep their debridement skills up to date for their scope of practice through continued CPD and training.
The Capability Framework for Integrated Diabetic Lower Limb Care (2019) is a useful guide to support clinicians in practicing within their scope, as not all healthcare professionals are trained to perform all forms of debridement. This reinforces the importance of a collaborative, multidisciplinary approach to ensure safe and effective patient care (Mayor et al, 2024; Vowden et al, 2011; Murphy et al, 2020).
High-risk patients and lower limb considerations
In the lower limb and feet, particularly in patients with diabetes, peripheral arterial disease (PAD), chronic limb-threatening ischaemia (CLTI), pyoderma gangrenosum and other high-risk areas or conditions, debridement must be performed with caution, due to anatomical complexity and an increased risk of complications. These complications can include:
- Risk of infection
- Necrosis
- Hospital admission
- In severe cases, amputation.
A full vascular assessment must be performed before initiating any method of debridement along with multidisciplinary decision-making (Lloyd Jones, 2015; Chadwick et al, 2014; Mayor et al, 2024).
The need for a debridement guide
A collaborative debridement guide was co-developed by Podiatry and Tissue Viability Nurses (TVNs) to support all nursing teams in the decision-making around debridement.
The number of complex, high-risk, hard-to-heal wounds is increasing across the healthcare system, and the consequences of complications can be life-changing for patients.
Decisions regarding when to debride – and when not to – are becoming increasingly complex, which can lead to adverse outcomes or delayed healing. The debridement guide provides clear, practical guidance on selecting the appropriate form of debridement for all anatomical areas of the body to provide safe and effective care to all patient groups. It also aims to reduce the risk of complications, improve multidisciplinary communication and enhance care planning. Ultimately, the guide creates standardisation, clinician autonomy and appropriate referrals, ensuring the right debridement is used for the right patient at the right time (Lloyd Jones, 2015; Chadwick et al, 2014; Mayor et al, 2024).
Overview of wound debridement modalities
There are many types of debridement to consider. Every patient will need a full holistic assessment to understand what factors will affect wound healing and what is the most safe and effective method of debridement for that individual patient. One of the most important assessments in lower limb wounds is vascular assessment.
There are a range of assessments that can be performed depending on the clinician’s level of skill; however, patients with known long-term conditions should be referred to specialist clinicians and services for advanced testing, in line with current National Institute for Health and Care Excellence (NICE) guidance (NG19; CG147) and the National Wound Care Strategy Programme (NWCSP).
This ensures that safe and effective treatment plans are implemented while reducing the risk of serious complications. Clinicians must also recognise their own level of competency and refer to specialists when the required debridement method falls outside their skill set, as outlined in the Capability Framework for Integrated Diabetic Lower Limb Care (2019).
Multiple methods of debridement may be used in combination, so a collaborative, multidisciplinary treatment plan is required (Mayor et al, 2024). Some debridement methods should be repeatable on a regular basis to optimise wound healing as part of a structured wound hygiene approach within care plans (Murphy et al, 2020).
There is no single standardised approach to debridement, which can make decision-making challenging for healthcare professionals. Mayor et al (2024) describe, in detail, the wide range of available methods, each associated with varying levels of invasiveness and risk.
Key considerations before selecting debridement
- Practitioner skill and competency
- Clinical setting
- Patient health status
- Social factors
- Patient consent
- Wound characteristics
- Mechanism of action
- Desired outcomes.
Forms of debridement include:
- Oxidative
- Autolytic
- Osmotic
- Enzymatic
- Chemical
- Chemo-mechanical
- Surfactant
- Biological
- Sharp
- Surgical
- Ultrasonic
- Hydrosurgical.
These methods may be used alone or in combination depending on the patient and wound assessment. Mayor et al (2024) also describe in detail the cautions and contraindications associated with these forms of debridement.
High-risk anatomical areas: cautions and contraindications
Mayor et al (2024) describe in detail the cautions and contraindications associated with different debridement methods. There are several patient co-morbidities and wound types that are not suitable for invasive forms of debridement due to the increased risk of complications, particularly in high-risk anatomical areas.
The potential complications that can occur include the risk of infection, pain and maceration (Gray et al, 2011). In some cases, invasive debridement is initially unsafe for certain anatomical areas; however, clinical status can change rapidly, particularly in relation to infection or vascular compromise, requiring urgent intervention for limb or life preservation (Mayor et al, 2024).
It is therefore imperative to perform in-depth holistic and vascular assessments prior to debridement to be able to provide safe, effective and patient-centred care.
Key cautions and contraindications
- Chronic limb-threatening ischaemia (CLTI) and peripheral arterial disease (PAD): Poor perfusion in feet and legs impairs healing and increases the risk of ulcers, infection, necrosis and amputation. ABPI <0.7 or toe pressures <50 contraindicate aggressive, invasive debridement
- Diabetes Mellitus: Neuropathy and ischaemia in the feet and legs increases the risk of ulcers, infection, necrosis, hospital admission and amputation
- Chronic Kidney Disease (CKD 4/5): Associated with poor healing, increased infection, necrosis and amputation risk
- Co-morbidities: Poor skin integrity and vascular fragility leading to hard-to-heal wounds in high-risk anatomical sites
- Palliative care
- Areas close to deeper anatomical structures: Tendon, joint, bone, nerves, major blood vessels
- High-risk areas: Face, neck, axilla, hands, feet, groin and genitalia
- Blood clotting disorders
- Patients with possible implants, vascular grafts and/or dialysis fistulas
- Pyoderma gangrenosum
- Neoplastic wounds, burns
- Malignancy: Anything suspected must be referred to dermatology on 2-week wait for urgent assessment.
This list is not exhaustive, and clinicians should apply clinical judgement in all cases, supported by the wider evidence base (Mayor et al, 2024; Gray et al, 2011; Vowden et al, 2011; Chadwick et al, 2014; NWCSP, 2023; Murphy et al, 2020).
Referral and escalation
All patients with foot ulcers should be referred to the Foot Protection Team (Podiatry) or the multidisciplinary foot team (MDFT) within one working day, in line with the NICE guidance (NG19; CG147) and NWCSP. This allows for collaborative shared care and tailored treatment plans including recommended debridement methods. Further onward referrals may be required to specialist services, including Leg Ulcer and Tissue Viability teams. Local agreed pathways should also be followed.
Development of the wound debridement guide
The development of the debridement guide arose from several opportunities. Podiatry was invited to support the delivery of debridement training to District Nursing teams, in collaboration with Tissue Viability and Leg Ulcer teams. This raised awareness of existing debridement guidance and its impact on wound dressing, wound hygiene and debridement selection for shared care patients.
There was some confusion over what dressings were suitable for high-risk patients in high-risk anatomical areas, especially regarding diabetic and vascular foot and leg ulcers. These patients are at increased risk of complications when inappropriate dressing or debridement methods are used. This highlighted the need for clear, multidisciplinary guidance to support clinical decision-making and ensure safe, effective wound care.
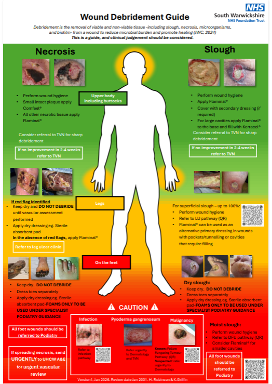
Podiatry and Tissue Viability teams initially collaborated to design a debridement pathway; however, this evolved into a more practical guide structured by anatomical areas using a Red-Amber-Green (RAG) rating system. This format provides direction while maintaining flexibility in clinical decision-making.
The guide includes suggested safe dressing options, supported by QR codes linking to local pathways for additional choices. It also incorporates prompts for specialist referral when more advanced debridement methods are required (see Figure 1).
The importance of collaboration in wound care
MDT working is increasingly recognised as fundamental for effective wound management given the complex and multifactorial nature of chronic wounds. Collier (2021) advocates collaborative working, emphasising that when professionals combine diverse skills to address patient needs, clinical outcomes are enhanced.
The contributions of podiatry specialists are particularly significant, with expertise in biomechanics, sharp debridement, offloading and custom orthotics (Boulton et al, 2018). Podiatrists often act as team builders and coordinators of care, working closely with Vascular, Microbiology and Tissue Viability teams (Bell, 2009).
A systematic review by Alaayashi and Alruwaili (2025) demonstrated that MDT working reduced healing times by approximately 25%, lowered amputation rates by approximately 35%, improved infection management and enhanced patient satisfaction. Similarly, multidisciplinary wound care protocols have been associated with fewer major amputations, faster healing, lower resource utilisation and reduced recurrence (Musuuza et al, 2021).
How we collaborated: A practical account
The Tissue Viability lead and the Podiatry Diabetes Lead came together during a Leading an Empowered Organisation (LEO) leadership course, where the debridement guide was developed as part of a quality improvement project. Numerous meetings took place during the design phase, and the guide was subsequently distributed for peer review across Podiatry, Tissue Viability and Leg Ulcer teams.
Progress was occasionally delayed due to winter pressures and workforce capacity challenges; however, all contributors remained mindful of competing clinical demands. The guide has since been approved by the Trust’s Pressure Ulcer Review Group and Audit and Operational Governance Group.
Initial rollout of the guide will target community-based podiatry, community nursing and leg ulcer teams. Implementation will be supported through existing meetings and scheduled training days throughout the year.
Clinical implications and recommendations
The debridement guide provides a clear RAG rating system for debridement selection based on anatomical risk, with the aim of reducing patient harm. It supports safe dressing and debridement choices to deliver holistic, patient-centred, effective wound care treatments, and timely referrals to specialists whilst reducing complications and harms.
Flaminal® (Flen Health), an enzyme alginogel, was selected as the primary debridement agent due to its triple-action properties:
- Continuous autolytic debridement
- Exudate management
- Antimicrobial protection.
Its unique formulation allows it to conform to uneven wound surfaces, cavities and sinuses, reducing dead space and supporting effective wound bed preparation.
Multidisciplinary collaboration has also helped streamline alternative dressing options where necessary, reducing confusion and ensuring adaptability across different clinical settings. Additional features of the guide include visual aids, QR-linked sub-pathways for diabetic foot and leg ulcers and escalation prompts for sharp debridement or specialist referral.
Once the debridement guide is launched and embedded within the Podiatry and Nursing teams, formal evaluation will be implemented to review its effectiveness. There will be consideration to include this into practice nurse training delivered by Podiatry teams in primary care. Where possible, wider dissemination across the Integrated Care System (ICS) would further support standardisation of wound care practice.
Conclusion
This collaboratively developed debridement guide demonstrates how a multidisciplinary approach can enhance wound care safety and effectiveness. By integrating anatomical risk, clinical judgement and product simplicity, the guide supports clinicians in delivering high-quality care across all anatomical sites.
Additionally, the guide encourages appropriate referral for sharp debridement and specialist services, ensuring that patients receive timely, safe, effective care tailored to their wound care needs.



