In clinical practice, structured risk assessment remains a key component of pressure ulcer prevention and treatment (Coleman et al, 2018). Risk factors are identified to detect patients who are susceptible to pressure ulcer development, enabling clinicians and nurses to create care plans that ensure seamless continuity of care for individual patients (Beldon, 2008). The aim is to identify people who are at risk of developing a pressure ulcer, and those not at risk, in order to plan and initiate individualised preventative interventions while making best use of resources.
International guidelines on pressure ulcer prevention and treatment recognise the burden of pressure ulcer development, on both patients and healthcare systems, and stress the importance of undertaking risk assessment on individuals (EPUAP/NPUAP/PPPIA, 2019). Clinical judgement and the recognition of specific risk factors are essential to refine risk assessment tools as part of a structured approach. Moreover, NICE (2014) recommends that a validated risk assessment tool (e.g. the Braden scale, the Waterlow score or the Norton risk-assessment scale) is used to support clinical judgement when assessing pressure ulcer risk in day-to-day practice.
Risk assessment in practice
There are over 40 pressure ulcer risk assessment scales available that vary in how they were developed (informed by literature/expert opinion or adapted from an existing scale) and the risk factors they cover (Stansby et al, 2014; Nixon et al, 2015). Some have more generic uses while others have been developed for specific populations e.g. paediatrics, end of life, orthopaedics, community and intensive/critical care. As there is a plethora of pressure ulcer risk assessment tools, there is an urgent need for standardised risk assessment that is easy and practical to use. Attendees were asked which risk assessment tools they currently use and alongside PURPOSE-T, Waterlow, Braden and Walsall were mentioned.
Risk assessment is a critical component of clinical practice, enabling timely and efficient identification of high-risk patients to allow clinicians to spend time and utilise resources more effectively. Most existing risk assessment tools use checklists and assign numerical values to various factors, with the resulting score being used as an indicator of pressure ulcer risk. These tools often stratify patients into categories, including low, medium or high risk. The most commonly used pressure ulcer risk assessment tools are the Braden Scale, the Norton Scale and the Waterlow Scale (Norton et al, 1962; Waterlow et al, 1985; Braden and Bergstrom, 1987; Hotaling and Black, 2021). Many existing assessment scales consider a diverse range of intrinsic (internal) factors, including mobility, activity, level of continence, chronic disease status, acute disease, nutrition, age, skin condition, mental status, medication and sensation (Beldon, 2008).
What is Purpose T?
Pressure Ulcer Risk Primary or Secondary Evaluation Tool (PURPOSE-T) is an evidence-based pressure ulcer risk assessment tool developed by the University of Leeds using robust research methods (CTRU Leeds, 2022). PURPOSE-T supports clinical decision-making and makes a distinction between three groups of patients: those not at risk of developing a pressure ulcer, those patients who have no pressure ulcer but who are at risk (requiring primary prevention) and those patients with an existing pressure ulcer/scar or who have had a pressure ulcer in the past (requiring secondary prevention and treatment; Nixon et al, 2015). Categories of PURPOSE-T risk assessment tool are colour-coded to indicate the most important risk factors as part of a three-step assessment process:
Step 1: Screening – to quickly screen out those clearly not at risk. It comprises assessment of mobility and skin status (including medical devices) as well as encouraging healthcare professionals to use their clinical judgement to highlight any other risk factors which significantly impact the individual patient.
Step 2: Full Assessment – incorporates the following evidence-informed items:
- Analysis of independent movement
- Detailed skin assessment
- Previous pressure ulcer history
- Medical devices
- Perfusion and nutrition
- Sensory perception and response
- Moisture due to perspiration, urine, faeces or exudate
- The presence of diabetes.
Step 3: Assessment decision based on step 2 and aided by colour-coding:
- Green: No pressure ulcer – not currently at risk
- Amber: No pressure ulcer – but at risk, requiring primary prevention
- Red: Pressure ulcer category 1 or above or scarring from previous pressure ulcer – requiring secondary prevention/treatment.
What makes Purpose T different?
PURPOSE-T is an evidence-based risk assessment tool that was developed using gold standard instrument development methods in a structured five-phase approach, incorporating a systematic review of pressure ulcer risk factors, a consensus study involving a mixed-speciality expert group and service users, conceptual framework development, cognitive pre-testing with clinical nurses and clinical evaluation in acute and community settings (Coleman et al, 2013; 2014; 2016; 2018). Guidance also recommends that a skin assessment is carried out and documented in those patients identified as being at risk of pressure ulcer development. This is recognised in PUPOSE-T, which requires a description of the skin in both the screening and assessment phases.
PURPOSE-T has already been implemented in early adopter trusts, both acute and community, and is ready for wider implementation across the National Health Service (NHS; Nixon et al, 2015). The National Wound Care Strategy Programme (NWCSP) will be recommending PURPOSE-T to healthcare professionals to prevent pressure damage and promote healing (NWCSP, 2022). The psychometric properties of PURPOSE-T have been tested with the tool demonstrating reliability, convergent validity and clinical usability when used by expert and ward/community nurses in secondary and community care settings (Coleman et al, 2018).
Existing risk assessment scales struggle to differentiate between patients with and without pressure ulcers and in clinical practice, risk assessment and skin assessment are often viewed as two separate processes (Coleman et al, 2014). In contrast, PURPOSE-T recognises the importance of skin status in the assessment of pressure ulcer risk and that visual examination of the skin may be influenced by context of care and level of patient dependency. By integrating skin assessment items, PURPOSE-T enables identification of vulnerable skin (e.g. dryness, paper thin and redness) or an existing pressure ulcer for improved risk assessment and subsequent care planning and delivery.
- Unlike other pressure ulcer risk assessment tools, which assign numerical values to various risk factors, no numbers or subjective levels of risk are involved in PURPOSE-T. PURPOSE-T drives clinicians towards critical thinking and individualised care for patients, giving them ‘permission’ to use their own clinical judgement. In comparison to existing risk assessment tools, PURPOSE-T (Nixon et al, 2015):
- Appropriate interventions are suggested in response to specific risk factors
- Includes pain as a risk factor and key indicator of pressure ulcer development
- Clearly distinguishes between primary and secondary prevention, so patients with an existing pressure ulcer or scarring are immediately allocated to a secondary prevention pathway, facilitating escalation of treatment and promoting healing
- Developed based on a systematic review of the risk factor evidence and pain cohort study, involving international and interdisciplinary experts and in partnership with service users.
Step 1: Screening
Colour code is integrated throughout PURPOSE-T, where blue indicates ‘no problem’, yellow indicates a potential impact on pressure ulcer risk, orange indicates risk and pink indicates that the patient has a pressure ulcer or ulcer scar (Coleman et al, 2018).
As part of the three-step assessment process, step 1 involves a screening stage assessing mobility status, skin status and clinical judgement. The purpose of the screening stage is to quickly identify those patients who are clearly not at risk and those patients with a potential risk or actual pressure ulcers who require a full assessment. If a yellow category is selected at screening stage, clinicians do not need to complete the remainder of the screening protocol and should instead proceed straight to the assessment stage.
An example of where clinical judgement would overrule PURPOSE-T would be in the case of a community patient who is independently mobile with normal skin but has frequent chest infections which impact on mobility. Clinicians should remember that risks during predicted periods of acute illness need to be mitigated against. A further example is where a patient appears to have normal skin but the skin on their arms is paper thin from long-term steroid inhaler use. Importantly, the determination of normal skin can be done through a conversation with the patient.
Healthcare professionals also need to consider how patients differ between day and night and to not immediately rule out any yellow boxes in the screening stage of PURPOSE-T. Day/night variations would include patients who mobilise independently during the day but stay in the same position all night. For example, an elderly patient who is on the community caseload for B12 injections and is housebound may still be independently mobile around the house and able to complete activities of daily living. This patient can be screened out, but clinicians need to remember the importance of information-giving as these patients are susceptible to becoming high risk very quickly with a short illness e.g. urinary tract infection (UTI) and chest infection.
Step 2: Full assessment
The full assessment stage of PURPOSE-T comprises analysis of independent movement, sensory perception, detailed skin assessment, previous pressure ulcer history, perfusion, nutrition, moisture and diabetes.
Importantly, the clinician should not just consider whether the patient can mobilise, but whether they actually do. The patient might have developed strategies to help them move around their home that may not be possible in an inpatient hospital setting e.g. holding onto furniture and organising objects in a way that provides easy access. Examples of reasons why patients might avoid mobilising (beyond physical reasons) include:
- Depression
- Pain (which can be weight related)
- Sedation
- Fear of falling.
When analysing independent movement, clinicians should bear in mind that while some patients are mobile in the day, they can struggle to move around in bed at night, possibly due to a previous surgery. Moreover, when assessing sensory perception, clinicians should remember that some patients cannot feel, or they can feel but are unable to respond appropriately to discomfort from pressure.
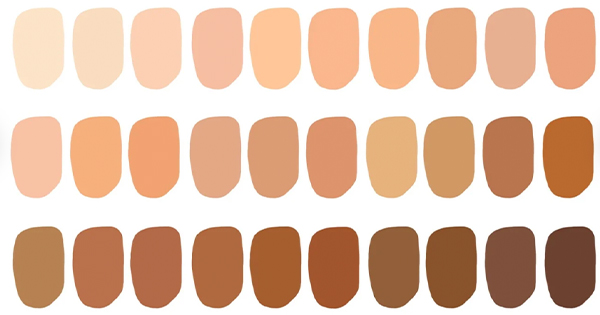
Another core element of PURPOSE-T is skin assessment and recording, especially with there being differences in skin assessment for people with dark skin tones (Coleman et al, 2018). A lack of early identification of skin changes can cause important signs to be missed, leading to skin and tissue breakdown and damage (Dhoonmoon et al, 2021). Consistent recording and terminology are essential to aid accurate assessment and diagnosis in all skin tones, to avoids biases that prevent individuals with dark skin tones from receiving accurate diagnosis and care.
Step 3: Assessment decision
The final step of PURPOSE-T requires consideration of step 2 responses to inform 1 of 3 assessment decisions, including ‘no pressure ulcer not currently at risk’, ‘no pressure ulcer but at risk’ and ‘pressure ulcer category 1 or above or scarring from previous pressure ulcer’ depending on the colour of the boxes ticked.
If any pink boxes are ticked, the patient has an existing pressure ulcer or scarring from a previous pressure ulcer (red group). If any orange boxes are ticked, the patient is at risk (amber group). If only yellow and blue boxes are ticked, the nurse must consider the risk profile, including risk factors, to decide whether the patient is at risk or not currently at risk (amber or green group). These three separate groups help determine which factors put the patient at risk. Where the patient fits into the red or amber group, the patient’s treatment should form part of an individualised pressure ulcer prevention/management care plan for specific risk factors. If in the green group, the patient should be reassessed as per pressure ulcer policy.
The importance of standardisation
Absence of standardised risk assessments, associated with falls and pressure ulcers, has been recognised by NHS Resolution as a key claim representing an episode of harm, with associated financial impact on the NHS and implications for patients, their families and the healthcare staff involved (NHS Resolution, 2022). As a prerequisite to implementation of an evidence-based pressure ulcer prevention and management protocol, standardisation of risk assessment may help to support communication between clinicians and organisations, ensuring relevant information is consistently shared and reducing the risk of error. Moreover, the NHS Long Term Plan lists improved digitisation as a key ambition for the service (NHS England, 2019). As healthcare systems undergo digital transformation and move towards wider digitisation of patient records, standardising wound management including risk assessment could help to improve patient outcomes.
Use of the tool in practice
Attendees of the session were invited to discuss in groups the following aspects to use of PURPOSE-T in practice:
- How would PURPOSE-T fit with your local protocols?
- Do you feel there would be any specific things to consider or any particular questions about use in certain specialist areas?
- How would this tool work in helping staff to identify appropriate equipment?
Several attendees shared that they have already embedded PURPOSE-T within their SSKIN care bundles to replace the Waterlow score; however, it was revealed during the discussion that a list of trusts that have already integrated PURPOSE-T would be useful to release. The group agreed that this would promote information sharing and allow tissue viability teams to network and offer support to one another. A further view raised was that this would save time and effort for areas that have yet to consider implementation of PURPOSE-T.
Participants agreed that protocols would need reviewing and possibly amending before PURPOSE-T can be implemented in their practices. An important reflection from the group was that PURPOSE-T generally fits with their local protocols but would need adapting for specialist areas and services provided by allied healthcare professionals. A view was raised that the tool looks different to existing risk assessment scales but already encompasses current assessments. There was widespread agreement that educating staff on the tool would be essential to facilitating change in practice.
When considering if there would be any specific things they would need to consider before using PURPOSE-T, attendees spoke of SystmOne (or other electronic patient records) and how PURPOSE-T would need to be integrated into the clinical computer system to enable patient information to be shared across healthcare organisations. Participants were also interested in hearing about whether PURPOSE-T could be used in specialist areas such as paediatrics, maternity and neonatal care. Some attendees asked for a clarification of definitions (e.g. vulnerable skin); however, following PURPOSE-T registration, healthcare professionals are provided with a user manual with instructions to support decision-making. A query was raised regarding the possibility of incorporating free text questions into PURPOSE-T to support individualised patient care. Attendees also agreed that consideration would need to be given to PURPOSE-T in the case of patients with dark skin tones and those with deep tissue injury.
In helping to identify appropriate equipment, the group agreed that PURPOSE-T would help tie in with equipment formulary and management as part of an integrated patient care process. It was discussed that there may be challenges getting healthcare professionals to convert and accept PURPOSE-T over risk assessments that are already being used in practice. Some participants argued that it is up to individual clinicians, and not PURPOSE-T, to use their clinical expertise and judgement to make decisions regarding equipment provision in line with local protocol; however, a general agreement was reached that clinical staff are currently so overburdened that they are worried about their own clinical judgement. The group were particularly keen to understand whether PURPOSE-T impacts on pressure ulcer equipment usage. Attendees agreed that therapist involvement would support identification of appropriate equipment alongside PURPOSE-T, for example occupational therapists who could help better assess the techniques, equipment and tools necessary for patients to live independently and safely.
Summary
PURPOSE-T is an evidence-based pressure ulcer risk assessment tool that identifies individuals at risk of developing a pressure ulcer and those with existing and previous pressure ulcers. It became apparent during the workshop that the tool is self-explanatory and becomes easier to use with familiarity. The RAG system (red-amber-green) approach aids decision-making and has numerous advantages over existing risk assessment scales, including lack of a numerical score, inclusion of pressure ulcer scar and pain as risk factors, addition of a detailed skin assessment and an efficient screening stage allowing for quick identification of patients not at risk.