Klein (2016) suggested that when the abdomen is closed primarily, we lose the window to the abdominal cavity. However, there are risks associated with keeping the abdomen open, such as fluid, protein and heat loss, as well as bowel adhesions and perforations.
There are several reasons to leave the abdomen open after surgery, these include:
- Abdominal compartment syndrome
- Peritonitis
- Easy access for return to theatre
- To allow infection to be treated
- Postoperative wound dehiscence
- High risk of fistula development (Fernández, 2016; Muhammad et al, 2016).
A fistula is an abnormal connection between two body parts. Patients are more prone to experience an enterocutaneous fistula when the abdomen is left open after surgery (Fernández, 2016). They are usually the result of an injury, surgery, or a consequence of infection, inflammation or malignancies (Heineman et al, 2015). Abdominal surgery can result in enterocutaneous or gastrointestinal fistulae. A postoperative gastrointestinal fistulae can occur after any abdominal procedure in which the gastrointestinal tract is handled (Falconi and Pederzol, 2002).
The aim of this article is to discuss the multifaceted management of these patients. A patient case will also be presented to illustrate the complexity of the open abdomen.
Best practice
The main goals of wound management for patients with an enterocutaneous fistula are control of fistula effluent and nutritional management (Heineman et al, 2015). SNAP is a recommended management plan for gastrointestinal fistulae to coordinate care and improve outcomes (Gribovskaja-Rupp and Melton, 2016). The SNAP approach encompasses development of a skin plan and management of sepsis if present (S), optimising nutrition, which may need to be parenterally administered (N), defining fistula anatomy (A) and planning a procedure to address the fistula (P). A multidisciplinary approach is essential (Gribovskaja-Rupp and Melton, 2016) and has been historically suggested to reduce mortality by 50% (Irving et al, 1985).
Skin surrounding the wound should be kept clean and dry and the application of a barrier cream is beneficial. Something to isolate the fistula from the wound and the output from the skin is required. This is sometimes described as pouching. The wound also needs to be supported with a dressing and this may need to be adapted to meet the needs of the patient.
Nutritional status is important for all patients with wounds. Optimising nutrition is crucial in this group of patients who are usually malnourished initially (Tang et al, 2020) and where the fistula itself is a source of fluid loss. A patient with a fistula with low fluid output requires approximately 20–30kcal per kilogram per day compared with a patient with a high output fistula who requires at least 25–35kcal per kilogram per day (Gribovskaja-Rupp and Melton, 2016). Dudrick et al (1999) stated that someone with an enterocutaneous fistula will require 1 to 2.5 times the energy of a healthy adult.
In order to establish the anatomy of the fistula, computed tomography (CT) scanning is recommended, although in patients who are critically unstable following their surgery this isn’t always possible.
A definitive procedure may be needed to address the fistula. Gribovskaja-Rupp and Melton (2016) suggest that this should be considered if there is no spontaneous closure of the fistula by 12 weeks after the multidisciplinary care package has been fully established (skin plan and managing any signs of sepsis, optimising nutrition and defining anatomy of the fistula from the SNAP approach). Soft tissue revision may be needed or a bowel resection or abdominal wall reconstruction. Non-surgical options include fibrin sealant, endoscopic clips or a fistula plug. Most of the evidence for these procedures is limited to case studies only.
Multidisciplinary working, discussions and planning are essential and will ensure optimisation of treatment. These patients usually experience long hospital stays and typically struggle psychologically following the pain and trauma they have endured.
Dressing options for the open abdomen
There have been various temporary solutions to support the open abdomen. A few include the Bogota Bag, Whitman Patch, abdominal closure system, wound packing, and negative pressure wound therapy (NPWT).
The Bogota Bag is a low-cost method for managing the open abdomen, being an open intravenous bag or sterile bag that is stapled or sutured to the skin (Demetriades, 2012; Muhammad et al, 2016). It doesn’t allow effective removal of excess fluid in abdominal oedema and is generally seen as a less favourable choice to other, more sophisticated options available. Despite this, they are often used as a temporary option to manage the open abdomen, as well as for longer periods (Muhammad et al, 2016).
The Wittmann Patch consists of hook-and-loop sheets pressed together to form a secure closure and peeled apart to allow access to the abdominal cavity (Fernández, 2016). The overlap can be adjusted to accommodate an increase or decrease in swelling.
The open abdominal NPWT kit uses a fenestrated sterile plastic drape over the base of the wound (for example the bowel) with foam over the top and adhesive to secure, to which the suction tubing is attached (Figure 1). This allows removal of fluid while bolstering the abdominal walls (Einav et al, 2021). While it increases the chances of closing the fascia, it is associated with a higher incidence of fistula formation (Einav et al, 2021). Before the development of the open abdominal kit, a similar vacuum packing technique was used consisting of a fenestrated plastic sheet with moist surgical towels to cover and drains attached to wall suction to remove fluid from the cavity (Fernández, 2016).
NPWT is a system whereby a wound is packed with foam or antimicrobial gauze (with the wound base lined in some cases) and sealed with adhesive film before suction is applied using a portable pump. Clinical benefits include improving perfusion to the area, reduction of oedema, removal of fluid, increasing cell proliferation and support to the wound edges and surrounding structures (Clough, 2012). However, caution must be taken to protect any underlying structures or organs and so it is not appropriate for use in some open abdominal cases. A Cochrane review on non-trauma patients concluded that it wasn’t clear whether NPWT has any benefit when compared with the Bogota bag and advised further research is needed (Cheng et al, 2022). The review included studies investigating any type of NPWT.
Case study
A 64-year-old lady underwent gastric bypass surgery, after which she deteriorated medically. A gastrojejunal anastomotic leak was identified. This required further surgery and washouts that were complicated by the anastomotic leak, an infective abdominal collection and a jejunal fistula.
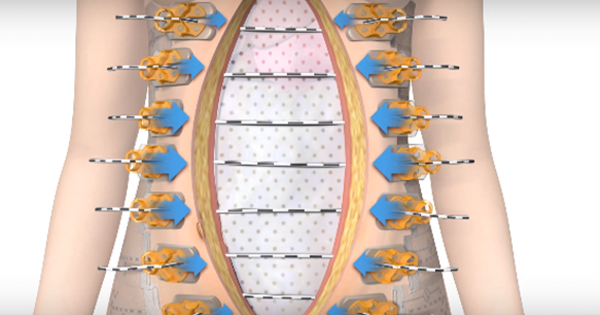
An ABRA® abdominal wall closure system (Figure 2) with foam NPWT (and a liner) was applied in theatre. The cords on the abdominal wall closure system were tightened every 24 hours and the NPWT was replaced approximately every other day. The patient was managed in critical care and was on total parenteral nutrition (TPN).
After five days the ABRA was removed and the fascia closed. Standard NPWT using foam and a liner was applied with little exudate within the following 24 hours. The fascia remained intact at the base of the wound with healthy granulating tissue across. However, there were concerns about pus oozing from the drain site. Wound care included washing with a wound irrigation solution for cleansing contaminated wounds (Octenilin wound irrigation solution), which can reduce any bioburden (Braun et al, 2013), as well as application of foam NPWT with a liner.
Approximately four to five days later there were concerns about possible bile visible at the base of the wound with no obvious leak. Wound assessment showed poorly perfused fatty wound edges. Due to concerns about the potential bile leak, the base of the wound was double lined. Antimicrobial gauze was applied to the wound edges with foam centrally.
A computerised tomography (CT) scan suggested the presence of a fistula, resulting in a decision to stop the NPWT and pack the wound with antimicrobial gauze covered with a superabsorbent dressing (Figure 3A). However, the surgeon requested NPWT to be restarted despite the fistula as there were concerns about wound management and non-healing in the absence of NPWT. The wound was irrigated with 0.9% sodium chloride and layers of dressings (in this case a hydrofibre dressing) were applied to the area where bile fluid appeared to be leaking to reduce suction to that area. NPWT with foam was then applied to the base of the wound with gauze to the edges and a liner used to the base, over the tension sutures (Figure 3B).
There were issues with fluid accumulation in the wound, so it was decided to use a channel drain to the inferior aspect of the wound. This was connected to the standard suction port using a Y connector and suction level was set low, at -60mmHg.
Following discussion with the surgeons, it was agreed to establish a better way of isolating the fistula. Several options were considered, but the depth of the fistula and its position tucked underneath the superior wall made this difficult. Some fistula isolation devices can be seen in Figure 4. Unfortunately, none of these could be positioned to isolate the area, although Heineman et al (2015) demonstrated techniques in which this could be achieved for some patients. In some cases, tubing, such as nasogastric tubes, have been used to segregate a fistula, but in this case the opening was too small and too deep within the wound wall to visualise and access with a tube. Finally, some isolation was achieved using a silicone pad, soaked in Octenilin before application.
The seal was better maintained using the silicone pad, which had sustained a wall to separate the fistula (Figure 5). NPWT was continued using this method to isolate the fistula and conservative sharp debridement was used to remove some non-viable tissue from the wound walls.
Almost two months after the gastrojejunal anastomotic leak was identified, the wound was filling with granulation tissue and making good progress. The patient was transferred to the ward and had began enteral feeding via a nasogastric tube (Figure 3C).
Unfortunately, there were some issues with food leaking into the wound and TPN was restarted while the patient had a nasojejunal tube sited. There were some concerns about recommencing parenteral nutrition as this was seen to be a backward step. However, as stated earlier, adequate nutrition is essential for healing, although enteral feeding will better protect the gut and prevent bacterial translocation than TPN (Tang et al, 2020). Enteral feed was recommenced a few days later.
Octenilin® was recommenced as the solution of choice to clean the wound due to the risk of contamination from food and bacteria entering through the fistula. Regular wound reviews alongside the surgeon continued with discussion about the plan.
As the wound became shallower, it was possible to try and isolate the fistula more definitively from the main wound and NPWT by applying a stoma bag. The Stoma Specialist Nurses were able to assist with options for trying to achieve this, although the fistula was unfortunately too deep to manage this way and the stoma bag repeatedly leaked.
The patient was commenced on oral fluids. Some of these were travelling through the fistula, but she was pleased to be able to have some water. Depression is common in patients with enteric fistulae (Heineman et al, 2015) and small activities can make a big difference to their outlook and quality of life.
NPWT was discontinued four months after the anastomotic leak was identified, and the wound was dressed with a dressing consisting of fibre packing and superabsorbent padding. Feeding via the tube continued and the patient was commenced on a pureed diet two weeks later after which the patient was able to go home with district nurse support (Figure 3D).
Conclusion
Early recognition of deteriorating wounds is needed and, the psychological effect these wounds have on patients is substantial. Managing an open abdominal wound is complex and with the added complication of a fistula, a structured patient focussed plan is needed using an approach such as SNAP. The success of treatment relies on optimising wound management, skin and managing sepsis, ensuring nutritional needs are addressed, establishing the anatomy of the fistula and planning a procedure to address the fistula.
A multidisciplinary approach is essential for successful healing. This should include tissue viability support, physiotherapy and consultant input among others. Furthermore, care plans should be mindful that each fistula and each patient will need treatment tailored to their individual needs.
Several dressing options are available, some more costly than others and some more sophisticated. More research into abdominal wall closure systems is needed to establish the most appropriate method for managing such complex wounds.